Wound Care Supply Selection: A 2026 Clinical Guide
- Qubit Technology
- Jun 10
- 9 min read

Wound care supply selection is the process of matching dressing types and clinical materials precisely to wound assessment findings to optimize healing outcomes. The difference between a wound that heals in weeks and one that stalls for months often comes down to whether the right dressing was chosen for the right reason. Frameworks like TIME (Tissue, Infection/Inflammation, Moisture, Edge) and the CLWK Wound Dressing Selection Quick Reference give clinicians and facility managers a structured path from assessment to supply decision. This guide applies those frameworks to help you select, standardize, and procure the most effective wound care products for your patient population.
What does wound care supply selection actually require?
Wound dressing selection starts with a complete wound assessment based on tissue type and treatment goals, not brand availability. This single principle separates clinical decision-making from habit-based purchasing, and it has measurable consequences for patient recovery. Facilities that anchor supply decisions to wound characteristics rather than vendor relationships report more consistent clinical outcomes and fewer unnecessary product substitutions. The assessment comes first. The supply follows.

How to perform a wound assessment that guides supply choices
A structured wound assessment covers four core elements: tissue type, exudate level, infection risk, and wound depth. Each element directly informs which dressing category is appropriate and eliminates guesswork at the point of care. Skipping any one element increases the risk of selecting a product that either dries the wound bed or saturates the periwound skin.
The TIME framework organizes these elements into a repeatable clinical process. Tissue type identifies whether the wound bed contains necrotic, sloughy, granulating, or epithelializing tissue. Infection and inflammation markers signal whether antimicrobial intervention is needed. Moisture balance determines whether the wound needs hydration or absorption. Edge assessment reveals whether the wound is progressing or stalled.
Clinicians should also evaluate skin lesion characteristics around the wound margin, since periwound maceration or excoriation directly affects which contact layer or secondary dressing is appropriate. Multidisciplinary input from wound care nurses, physicians, and pharmacists strengthens assessment accuracy, particularly for complex or chronic wounds.
Key assessment parameters to document at every dressing change:
Tissue type: necrotic, sloughy, granulating, or epithelializing
Exudate: none, low, moderate, or high, plus color and odor
Wound dimensions: length, width, and depth in centimeters
Periwound skin: intact, macerated, erythematous, or fragile
Pain level: at rest and during dressing changes
Signs of infection: increased exudate, malodor, friable granulation, or erythema
Pro Tip: Document wound status at every dressing change, not just scheduled assessments. Most infection signs become apparent during dressing changes, so supply selection must support accurate detection and documentation at these times.
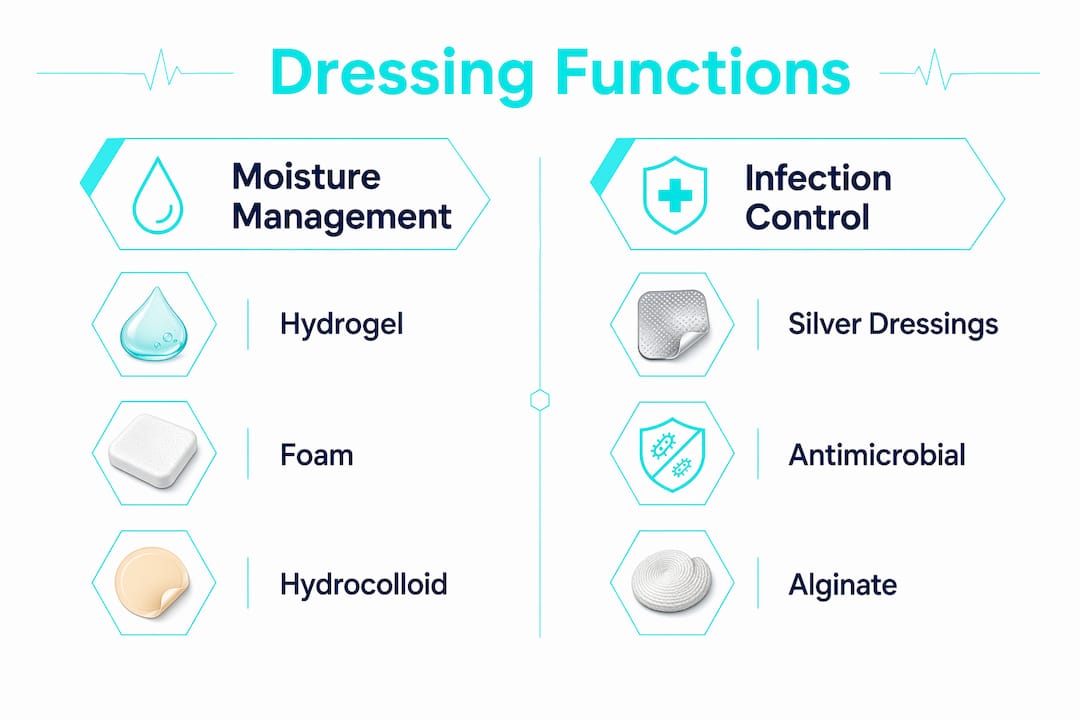
What are the main dressing categories and their clinical functions?
Dressing categories are defined by their primary moisture management function. Moisture balance categories include dressings that add moisture, maintain moisture, or absorb moisture. Understanding this functional taxonomy is more useful than memorizing brand names, because it allows clinicians to substitute within a category when a specific product is unavailable.
Dressing category | Primary function | Best suited for |
Hydrogel | Adds moisture to dry wound bed | Necrotic or dry sloughy wounds |
Hydrocolloid | Maintains moisture, light absorption | Shallow wounds with low to moderate exudate |
Foam | Absorbs moderate to high exudate | Granulating wounds with significant drainage |
Alginate | High-volume absorption, hemostatic | Heavily exuding or bleeding wounds |
Silver/antimicrobial | Manages bioburden, reduces infection | Locally infected or high-bioburden wounds |
Silicone contact layer | Maintains moisture, atraumatic removal | Fragile skin, painful wounds, epithelializing tissue |
Transparent film | Maintains moisture, visual monitoring | Superficial wounds, IV sites, low exudate |
Foam dressings are the workhorses of most outpatient formularies because they manage moderate to high exudate without requiring frequent changes. Silicone contact layers are particularly valuable for patients with fragile or aging skin, where adhesive trauma at dressing removal is a documented complication risk. Hydrocolloids self-adhere and create a moist healing environment, making them appropriate for pressure injuries at Stage II. Alginates are derived from seaweed and convert to a gel on contact with wound fluid, providing both absorption and a moist interface.
Pro Tip: When a wound transitions from high to low exudate during healing, switch dressing categories accordingly. Continuing a high-absorbency foam on a nearly healed wound will dry the wound bed and delay epithelialization.
How to match wound characteristics to the best wound care supplies
Translating assessment findings into supply decisions follows a logical sequence. The steps below reflect current best-practice decision frameworks and apply across acute, post-surgical, and chronic wound types.
Identify the dominant tissue type. Necrotic or dry sloughy tissue requires a hydrogel or autolytic debridement agent before any other dressing is appropriate. Applying a foam over a necrotic wound bed does not address the underlying barrier to healing.
Classify exudate volume. Low exudate calls for hydrocolloids or silicone contact layers. Moderate exudate suits foam dressings. High exudate requires alginates or superabsorbent dressings. Mismatching exudate level to dressing absorbency is the most common cause of periwound maceration.
Assess infection risk before selecting antimicrobial products. Silver dressings are indicated only for wounds with clinical signs of local infection, with a reassessment window of 10 to 14 days. Routine use of silver dressings on clean wounds is not clinically justified and adds unnecessary cost.
Determine dressing change frequency by function, not calendar. Change dressings earlier if the dressing fails, the wound shows maceration, or saturation occurs before the expected wear time. Fixed-schedule changes ignore wound status and increase both trauma and cost.
Identify infection markers during each dressing change. Local infection indicators include increased exudate, malodor, pain, friable granulation tissue, and periwound erythema. When two or more markers are present, escalate to an antimicrobial dressing and reassess within 10 to 14 days.
Build a “time to escalate” trigger into your supply policy. If a wound shows no measurable healing progress after two weeks on the current regimen, the supply selection and overall treatment plan require formal reassessment. This trigger prevents chronic wounds from stalling indefinitely on an ineffective product.
Adjust supply choices as the wound progresses. Healing wounds move through phases, and the dressing that was appropriate for a heavily exuding wound at week one is rarely appropriate at week four. Reassessment at each dressing change should prompt a category review, not just a product reorder.
How to build a formulary that simplifies procurement
Formulary standardization is the most effective organizational strategy for reducing supply complexity without compromising clinical coverage. Most outpatient facilities cover 90% of wound care needs with four dressing categories: foam, silicone contact layers, hydrocolloids, and antimicrobial dressings. This finding means that a facility stocking dozens of wound care SKUs is almost certainly carrying redundant products that add cost and decision fatigue without improving outcomes.
A well-designed formulary organizes products by function rather than brand. Within each category, tiered formularies with category-level alternates reduce decision fatigue and support substitution without expanding SKU counts. This structure also protects against supply chain disruptions, since clinicians can substitute within a category without retraining or clinical risk.
Procurement policies should incorporate clinical decision frameworks directly. When a purchase order for silver dressings is placed, the policy should require documentation of clinical indication. This creates a stewardship loop that controls cost and prevents inappropriate use. Review the essential surgical supply categories relevant to your facility type to identify gaps in your current formulary.
Additional considerations for facility-level procurement:
Staff education: Formulary changes require training. Clinicians who understand the functional rationale for a dressing category adopt new products more reliably than those given a substitution list without context.
Outcome monitoring: Track wound healing rates, infection rates, and dressing change frequency by product category. This data identifies which supplies are performing and which are being used outside their intended indication.
Supply chain redundancy: Identify at least one alternate product per category and pre-qualify it with clinical staff before a shortage occurs.
Storage compliance: Proper medical supply storage conditions affect dressing integrity. Hydrogels and alginates are particularly sensitive to temperature and humidity extremes.
For facilities using negative pressure wound therapy (NPWT), supply selection extends beyond dressings. NPWT procurement requires staff training on dressing change frequency, seal integrity, and complication avoidance to maintain clinical effectiveness. NPWT supplies should be managed as a separate formulary category with dedicated training protocols.
Common mistakes that undermine supply selection accuracy
Even experienced clinicians fall into predictable patterns that compromise wound care supply decisions. Recognizing these errors is the first step toward correcting them at both the individual and facility level.
Brand familiarity over clinical need. Defaulting to a familiar product regardless of wound characteristics is the most widespread error in wound care procurement. A foam dressing from a trusted vendor is still the wrong choice for a dry necrotic wound.
Routine antimicrobial use without indication. Silver dressings are stewardship-sensitive and should be used with clinical justification and time-limited trials. Applying them prophylactically on clean wounds drives cost up and provides no clinical benefit.
Fixed-schedule dressing changes. Changing dressings every Monday and Thursday regardless of wound status ignores functional failure points and increases unnecessary trauma to the wound bed.
Ignoring periwound skin condition. A dressing that is appropriate for the wound center may be damaging the surrounding skin. Periwound maceration, stripping, or contact dermatitis all require a supply adjustment.
Under-documentation at dressing changes. Incomplete records prevent accurate trend analysis and make it impossible to identify whether a supply change is producing results.
Pro Tip: Build a brief wound status checklist into your dressing change documentation template. Clinicians who complete a structured checklist at each change are significantly less likely to miss early infection signs or delay supply escalation.
Key takeaways
Effective wound care supply selection requires matching dressing categories to wound assessment findings using structured frameworks like TIME, not brand preference or fixed schedules.
Point | Details |
Assessment drives selection | Start every supply decision with tissue type, exudate level, infection risk, and wound depth. |
Moisture function defines categories | Classify dressings as adding, maintaining, or absorbing moisture to guide substitution and procurement. |
Silver dressings require justification | Use antimicrobial dressings only for wounds with confirmed local infection signs and reassess within 10 to 14 days. |
Formulary standardization reduces complexity | Four functional categories cover 90% of outpatient wound care needs and reduce SKU proliferation. |
Change frequency follows wound status | Dressing changes should be triggered by functional failure or wound status, not a fixed calendar schedule. |
Why structured selection is the only defensible approach
After years of working with healthcare facilities on supply procurement, the pattern I see most often is this: a facility has 40 wound care SKUs on its formulary, clinicians use 8 of them consistently, and nobody can explain why the other 32 are there. That is not a supply problem. It is a decision-making problem that happens to show up in the supply catalog.
The facilities that get wound care right are the ones that treat supply selection as a clinical discipline, not a purchasing function. They build their formularies around wound characteristics, train staff on functional dressing categories, and review outcomes data quarterly. They also treat antimicrobial stewardship in wound care with the same seriousness they apply to antibiotic prescribing. Silver dressings are not a default upgrade. They are a time-limited intervention with a defined reassessment window.
The other thing I have observed is that supply chain resilience is almost always an afterthought until a shortage hits. Facilities with category-level alternates pre-qualified in their formulary handle disruptions without clinical impact. Facilities without them scramble, and patients sometimes receive suboptimal dressings simply because nobody planned for substitution.
The bottom line is that wound care supply selection is a clinical governance issue as much as a procurement one. Facility managers and wound care leads who treat it that way consistently outperform those who leave it to individual clinician preference.
— QB
Stock your formulary with supplies that meet clinical standards
Queenssurgical supplies healthcare facilities across the Americas with wound care products that meet clinical and safety standards for professional use. The catalog includes dressings, contact layers, and periwound skin protection products, including DynaShield Skin Protectant Cream, which supports periwound skin integrity during extended dressing wear. For infection control at dressing changes, nitrile examination gloves provide reliable barrier protection. Queenssurgical offers both wholesale and retail purchasing options, making it practical for individual clinicians and large facility procurement teams alike. Browse the full catalog to identify products that align with your formulary categories and clinical protocols.
FAQ
What is wound care supply selection?
Wound care supply selection is the clinical process of choosing dressings and materials based on wound assessment findings, including tissue type, exudate level, and infection risk. It follows structured frameworks like TIME rather than brand preference or habit.
How do I choose the right wound dressing type?
Match the dressing category to the wound’s moisture needs: hydrogels for dry wounds, foams for moderate to high exudate, and silicone contact layers for fragile or epithelializing tissue. Antimicrobial dressings are appropriate only when local infection signs are present.
How often should wound dressings be changed?
Dressing change frequency should be dictated by dressing function and wound status, not fixed time intervals. Change earlier if the dressing is saturated, the wound shows maceration, or signs of infection appear.
When are silver antimicrobial dressings indicated?
Silver dressings are indicated for wounds with clinical signs of local infection such as increased exudate, malodor, or periwound erythema. Current guidance recommends a reassessment window of 10 to 14 days to evaluate response and discontinue if infection resolves.
How does formulary standardization improve wound care procurement?
Standardizing by dressing function rather than brand reduces SKU complexity and supports consistent clinical use. Most outpatient facilities cover 90% of wound care needs with four functional categories, which simplifies procurement and reduces decision fatigue for clinical staff.
Recommended
Comments